Fat necrosis is a common benign lesion of the breast. It is resulting from necrosis of the fat cells as result of a vascular ischemia. It is usually related to blunt trauma, previous biopsy, lumpectomy, reduction mammoplasty or radiation therapy [1].
In postoperative breast the presence of architectural distortion, post-treatment edema and increased breast density in digital mammography and breast ultrasound may impair detection of postoperative malignant recurrence [2].
Post contrast MRI of breast has an important role in evaluation of the postoperative breast lesions, like distortion that seen in mammographic follow up of the post-operative breast [3].
The diagnosis of postoperative fat necrosis is considered as a challenging imaging pitfall. Once fat necrosis is diagnosed it is categorized as BI-RADS 2 or BI-RADS 3 category.
In post contrast breast MRI the margins and the enhancement pattern of fat necrosis may be indistinguishable from recurrent malignant tumor. The clue for the diagnosis of postoperative fat necrosis in breast MRI is the presence of fat on T1WI [4].
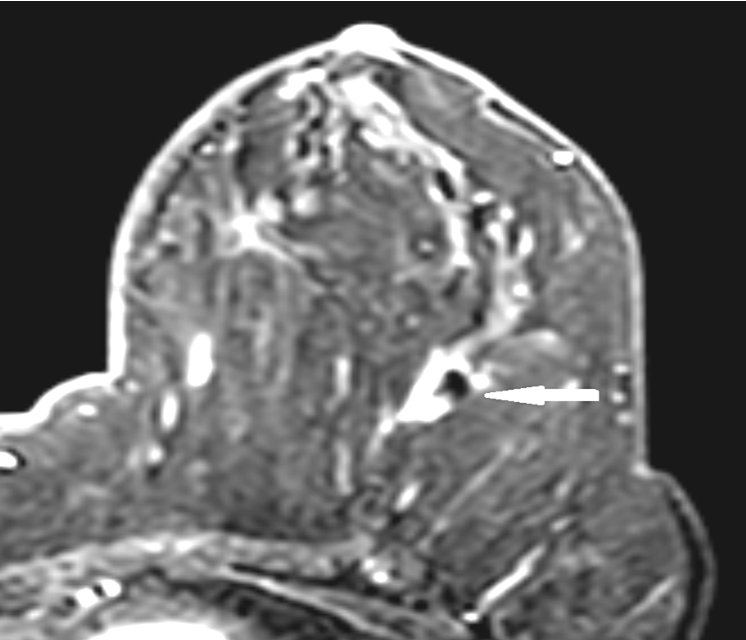
The patient performed breast MRI and there was a lesion in the operative bed of the left breast. In non-fat saturated T1 images the fat within the lesion had the same signal of the surrounding breast parenchymal fat and it was surrounded by a hypointense area of architectural distortion. In short T1 inversion recovery (STIR) images the fat within the lesion was low signal like the normal surrounding parenchymal fat.
After post contrast study the fatty lesion showed homogeneous thick rim enhancement and this was in agreement with the commonest enhancing pattern of fat necrosis reported by Daly et.al. [1]. The architectural distortion area surrounding the lesion showed no significant enhancement in post contrast study and this excludes the presence of post-operative malignant residual or recurrence.
The time signal intensity curve of the enhancing part of the lesion showed slow rise in early phase with plateau delayed phase (type II borderline plateau curve). This pattern was reported by Chala et.al. he noted that fat necrosis enhancement patterns may be similar to those seen in malignant lesions and the degree of this enhancement depends on the degree of the associated inflammatory process [5].
In diffusion weighted images (DWI) the lesion and its surrounding architectural distortion showed free diffusion with high apparent diffusion coffiecient (ADC) value denoting its benign nature and this match with Mansour et.al. study they concluded that MR diffusion increases the MRI diagnostic value in differentiation between postoperative benign and malignant breast lesions [6].