Targeted ultrasound for the diagnosis of mammographic masses with obscured borders
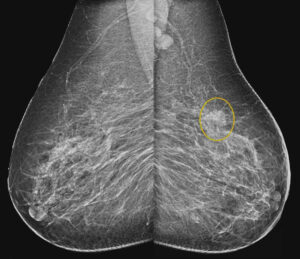
Figure 1: A (mediolateral oblique) and B (craniocaudal) mammographic images showed irregular shaped mass with obscured margins in the upper outer quadrant of the left breast associated with enlarged ipsilateral axillary nodes (noted at the medio lateral oblique view). Concomitant left breast diffuse skin and trabecular thickening.
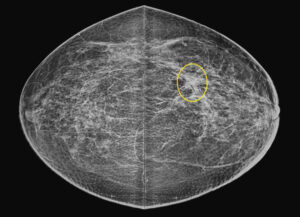
Figure 1: A (mediolateral oblique) and B (craniocaudal) mammographic images showed irregular shaped mass with obscured margins in the upper outer quadrant of the left breast associated with enlarged ipsilateral axillary nodes (noted at the medio lateral oblique view). Concomitant left breast diffuse skin and trabecular thickening.
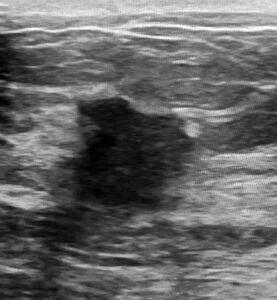
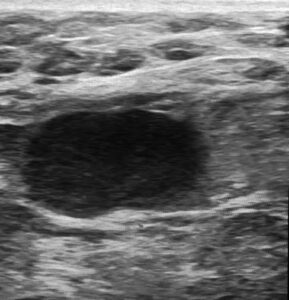
Figure 2: Ultrasound image showed an irregular shaped hypoechoic mass with spiculated borders and posterior shadowing in the upper outer quadrant of the left breast.